Neonates and infants aged <8 months whose mothers were not vaccinated at least 2 weeks before giving birth, or who are at increased risk of severe disease, are recommended to receive passive immunisation with a long-acting RSV-specific monoclonal antibody
A single dose of the RSV vaccine Abrysvo is recommended for all women in each pregnancy from 28 weeks gestation, as the first opportunity to protect their infant. See Pregnant women are recommended to receive an RSV vaccine during pregnancy to protect the infant. Do not give RSV vaccine Abrysvo to infants and young children.
Nirsevimab is a long-acting RSV-specific monoclonal antibody that is recommended for infants who were born:
- to women who did not receive RSV vaccine during pregnancy
- <2 weeks after the mother received RSV vaccine during pregnancy
Nirsevimab is also recommended for the following infants after assessment by their treating doctor to confirm potential clinical benefit:
- infants with risk conditions for severe RSV disease, regardless of maternal vaccination (see Table. Conditions associated with increased risk of severe RSV disease in infants and young children)
- infants born to mothers with severe immunosuppression, where the immune response to maternally administered RSV vaccine was impaired (see People who are severely immunocompromised)
- infants who have lost effective passive immunisation:
- those whose mothers have received RSV vaccine in pregnancy but who have subsequently undergone a treatment after birth, such as exchange transfusion, cardiopulmonary bypass or extracorporeal membrane oxygenation, that may lead to loss of maternal antibodies, OR
- those who have already received nirsevimab but have subsequently undergone one of the procedures above (noting this would be a repeat dose of nirsevimab)
See Figure. Flowchart to guide which infants should receive nirsevimab in their 1st RSV season.
Nirsevimab is not recommended for infants during the first 6 months of life if:
- the infant’s mother received RSV vaccine at an appropriate time during pregnancy, AND
- the infant does not have a risk condition for severe RSV disease
Figure. Flowchart to guide which infants should receive nirsevimab in their 1st RSV season
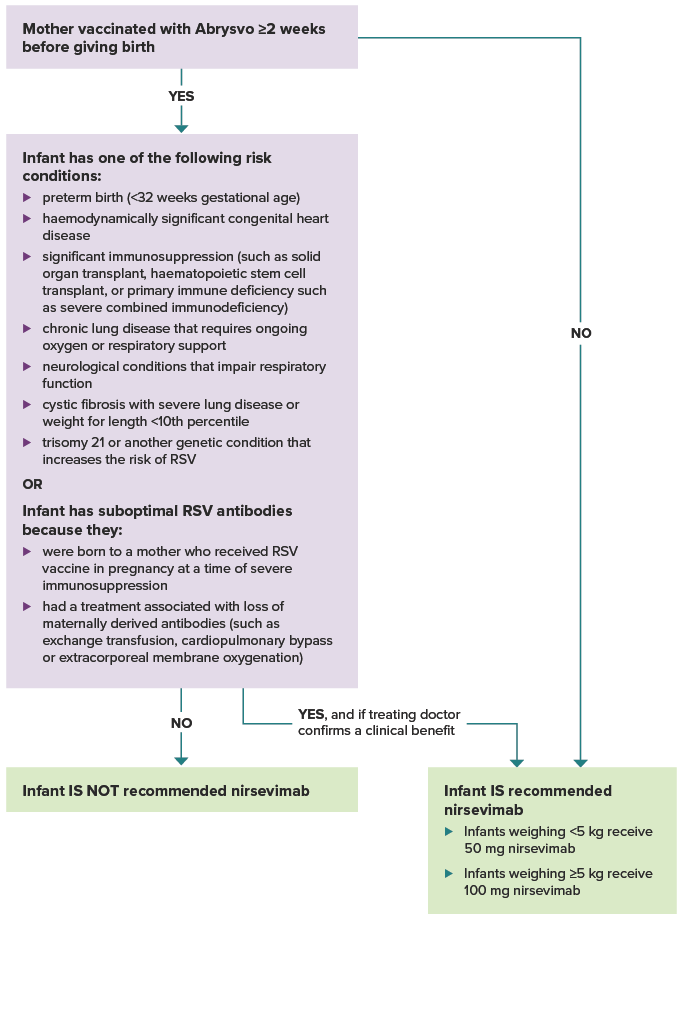
Was the mother vaccinated with Abrysvo at least 2 weeks before giving birth? If yes, and the infant does not have one of the risk conditions or conditions for suboptimal antibodies listed below, the infant is not recommended nirsevimab.
If the mother was not vaccinated at least 2 weeks before delivery, the infant is recommended nirsevimab. Infants weighing less than 5 kg receive 50 mg nirsevimab. Infants weighing 5 kg or more receive 100 mg nirsevimab.
If the mother was vaccinated at least 2 weeks before delivery, does the infant have one of the following risk conditions: preterm birth (<32 weeks gestational age), haemodynamically significant congenital heart disease. significant immunosuppression (such as from malignancy, solid organ transplant, haematopoietic stem cell transplant, or primary immune deficiency such as severe combined immunodeficiency), chronic lung disease that requires ongoing oxygen or respiratory support, neurological conditions that impair respiratory function, cystic fibrosis with severe lung disease or weight for length <10th percentile, trisomy 21 or another genetic condition that increases the risk of RSV? Or, does the infant have suboptimal RSV antibodies because they were born to a mother who received RSV vaccine in pregnancy at a time of severe immunosuppression, or they had a treatment associated with loss of maternally derived antibodies (such as exchange transfusion, cardiopulmonary bypass or extracorporeal membrane oxygenation)? If the infant does not have a risk condition or suboptimal RSV antibodies, they are not recommended nirsevimab. If the infant does have a risk condition or suboptimal RSV antibodies, they are recommended nirsevimab if their treating doctor confirms a clinical benefit.